TL;DR: Childhood myopia (nearsightedness) often worsens each year as kids’ eyes grow. Unchecked, it can lead to high prescriptions and higher risks of serious eye problems in adulthood. Thankfully, evidence-based interventions can slow myopic progression by ~30–60%, including low-dose atropine eye drops, overnight corneal reshaping (orthokeratology), special multifocal contact lenses, and new defocus spectacle lenses (e.g. MiYOSMART, Stellest). Increasing outdoor time and managing near work also help. Opticians can play a key role in explaining these options to parents in clear, reassuring language. This guide covers how each method works, effectiveness (e.g. many cut eye growth in half), ages and follow-up, plus a handy comparison table. Always ensure a comprehensive eye exam guides any myopia management plan. A friendly disclaimer: this post is educational, not medical advice – families should consult an eye care professional for personalized recommendations.
A Parent’s Story: “Why Are My Child’s Glasses Getting Stronger?”
“Last year my 8-year-old needed her first glasses at -1.00. Now she’s -1.75 in one eye. I’m worried – will it just keep getting worse? The optometrist mentioned treatments to slow it down, like special drops or lenses. I left feeling overwhelmed. I want to do what’s best, but it’s all new to me.”
If you’ve heard a parent share a similar concern, you’re not alone. Childhood myopia (nearsightedness) is on the rise worldwide . Many kids’ eyeglass prescriptions “jump” by -0.50 to -1.00 diopter or more per year during school-age growth spurts. Parents naturally worry how bad it might get. As an optician, you can reassure families that myopia progression can be managed. Several science-backed options can slow down eye elongation, meaning a child’s prescription would still change, but much more slowly than without treatment.
In this guide, we’ll first explain what myopia is and why it tends to worsen in children. Then we’ll break down the main myopia control tools available today – from low-dose medicated eye drops to specialized contacts and glasses – including how they work, how effective they are, and the pros/cons. We’ll keep the language parent-friendly while providing the evidence and numbers you need to feel confident in each option. By the end, you’ll have practical talking points to empower families in making informed decisions. Let’s dive in!
What Is Childhood Myopia and Why Does It Progress?
Myopia is when the eye grows too long (front to back) for its focusing power . Light from distant objects then focuses in front of the retina (the back of the eye) instead of on it, making far-away things look blurry (while near vision often remains clear). A child with myopia might squint to see the board at school but read a book up close just fine. The common fix is prescription glasses or contact lenses that diverge light rays, moving the focus onto the retina. However, standard single-vision lenses only correct vision – they don’t address the underlying eye growth. The eye may continue lengthening, leading to a stronger prescription each year.
Why do kids’ eyes keep getting more nearsighted? Genetics play a role (if both parents are myopic, a child is at higher risk), but environmental factors are big contributors. Modern children spend long hours on near work (reading, screens) and relatively less time outdoors. The theory is that extended close focusing and less daylight exposure can stimulate the eye to elongate abnormally . Myopia often starts in early grade school and tends to progress fastest in childhood and early teens as the eye is growing. It usually stabilizes by the late teens to early 20s once the eye reaches adult size.
Crucially, the faster and earlier myopia progresses, the higher the final prescription might end up. For example, a child who starts at -1.00 at age 8 and progresses -1.00 per year could be around -6.00 by age 14. In contrast, slowing that progression by half could keep them closer to -3.00 at 14 – a big difference in both daily life and future risks. This is why early intervention is important.
Why Does Myopia Control Matter? (Beyond Just Thicker Glasses)
Slowing myopia isn’t only about keeping glasses thinner (though children certainly appreciate not having super thick lenses!). The higher the myopia, the greater the risk of serious eye health issues later in life. An eye that grows very long can stretch and weaken the retina and other structures. High myopia (often defined as -6.00 or worse) significantly increases the chance of retinal detachment, early cataracts, glaucoma, and myopic macular degeneration – changes in the retina that can permanently damage vision . In fact, high myopia is becoming a leading cause of visual impairment worldwide .
By reducing how much the eye elongates, myopia control treatments aim to lower these long-term risks. For instance, slowing a child’s progression so they end up at -4.00 instead of -8.00 could cut their lifetime risk of myopic maculopathy by an estimated 40% . Even a 1 diopter less of myopia makes a meaningful difference in eye health outlook .
From a functional standpoint, managing progression means a child will have better uncorrected vision (handy if they ever forget glasses) and more options for things like sports (since extremely high myopes may struggle even with contacts). Down the road, moderate myopia is also easier to treat with refractive surgery if desired; very high myopia sometimes can’t be fully corrected with LASIK/PRK.
In short, myopia control isn’t about “curing” myopia – your child will still likely need glasses or contacts – but it’s about protecting their future eye health and minimizing how strong their prescription gets. It’s an investment in their visual well-being. And fortunately, we now have several proven tools to help do this.
Key Myopia Control Approaches: Below we introduce the main management options available today. Each is a bit different – some are eye drops used nightly, others are special lenses worn either overnight or during the day. Sometimes a combination is used (for example, orthokeratology plus atropine). The best choice depends on the child’s age, prescription, lifestyle, and how comfortable the family is with each method. We’ll go through them one by one.
Myopia Control Options: Overview of Today’s Evidence-Based Treatments
Low-Dose Atropine Eye Drops (Nightly)
What it is: Atropine is a medicated eye drop derived from the belladonna plant (in much lower concentration than used to dilate eyes in exams). In low doses (typically 0.01% to 0.05%), atropine can slow the progression of myopia in children. Parents put one drop in each eye at bedtime. The exact way it works is still studied, but atropine seems to act on growth signals in the eye to reduce excessive elongation.
Effectiveness: Robust studies show low-dose atropine significantly slows myopia progression. A meta-analysis of trials found that over 1 year, 0.01% atropine slowed myopia by about 27%, while 0.025% and 0.05% drops slowed it by roughly 43% and 67% respectively versus placebo . In other words, higher concentrations have somewhat greater effect on average. However, even the ultra-low 0.01% (often called “atropine sulfate 0.01%”) can cut annual progression by about 0.5 diopter less than without treatment . Over 2–3 years, that adds up. Some long-term trials (e.g. in Singapore and Hong Kong) have shown around 50% total reduction in progression with nightly atropine compared to controls . Importantly, multiple studies found no huge difference in final outcomes between 0.01% and higher doses, especially once you account for “rebound” after stopping drops . This is why many doctors start with 0.01% as first-line – it works well for many kids with minimal side effects.
Age suitability: Atropine can be used in quite young children (even 5–6 year olds and up). It’s often recommended for younger myopic kids or any child showing fast progression. The younger the child, the more years they have ahead for myopia to worsen, so early intervention helps. Drops are easy to use even if a child isn’t ready for contact lenses. Pediatric ophthalmologists commonly prescribe low-dose atropine for elementary-age children.
Pros: Easiest routine – just one drop nightly at home. It doesn’t rely on the child wearing a special lens during the day. High effectiveness (~50% slowing on average ). Minimal impact on day-to-day life (no activity restrictions). Can be combined with glasses or contacts. Great for kids too young or hesitant to try contact lens options.
Cons: It’s a long-term treatment – typically given for 2–3 years or more during the high-risk growing years. There is no permanent “cure”; myopia might continue to progress once treatment stops (possibly with a temporary rebound, though low doses have minimal rebound effect ). So, families must be committed to nightly drops for several years. Atropine is not a commercial over-the-counter medication for myopia in most countries; it’s usually prepared by a compounding pharmacy, which can make it relatively costly (though still generally a few hundred USD per year, far less than the cost of high-index lenses for very strong prescriptions down the line). Finally, some kids (and parents) may initially be nervous about putting drops in the eyes.
Side effects: At the low concentrations used for myopia, side effects are mild and uncommon. Atropine causes pupils to dilate slightly and can reduce focusing ability at near. With 0.01% these changes are tiny – most kids don’t notice any symptoms . At 0.05%, a minority might have a bit of light sensitivity in bright sun (wearing sunglasses/hat helps) or need a weak reading glasses for prolonged near work, but in studies children tolerated 0.05% well overall . Rarely, allergic conjunctivitis can occur (red/itchy eyes) – if so, the drops are discontinued. Low-dose atropine does not affect eye color (that was old high-dose atropine used chronically in the XIX century!). Overall, 0.01% atropine is considered as safe as placebo with no significant adverse effects in studies . (See the Safety Snapshot box for more.)
Follow-up: A typical schedule is an eye exam every 6 months to measure changes in prescription and axial length (eye length). If progression has slowed to an acceptable rate (e.g. from -1.00/year to -0.25/year), the current regimen is kept. If a child is still progressing fast even on 0.01%, the doctor might increase the dose (to 0.025% or 0.05%) for greater effect . After ~2 years, some clinicians attempt a trial off the drops to see if progression has naturally slowed; if the myopia “speeds up” again, treatment is restarted (this was the approach in the Singapore ATOM studies). In all cases, consistent nightly dosing is important – skipping drops frequently can reduce effectiveness.
Orthokeratology (Overnight Corneal Reshaping Lenses)
What it is: Orthokeratology, or ortho-k, uses specially designed rigid gas-permeable contact lenses worn overnight to gently reshape the cornea. The lens is custom-fitted to the child’s eye curvature. As they sleep, the lens flattens the central cornea by a tiny amount, which corrects the nearsighted prescription by morning. The child removes the lenses upon waking and can see clearly all day without glasses or contacts. It’s like temporary laser eye surgery that you repeat each night! Importantly for myopia control, ortho-k lenses also create a focused image on the peripheral retina that is thought to slow the stimulus for the eye to elongate .
Effectiveness: Orthokeratology is one of the most established myopia control methods, with over 20 years of research. Studies and meta-analyses show ortho-k slows axial eye growth by roughly 40–60% compared to wearing regular single-vision glasses . In practical terms, children using ortho-k tend to have about 50% less increase in prescription each year than those in standard lenses. For example, a 2-year trial found eye elongation of 0.36 mm in the ortho-k group versus 0.63 mm in controls – a ~43% reduction in growth . Another study reported an average 0.27 mm annual axial growth with ortho-k vs 0.38 mm with glasses, translating to ~0.25 D less myopia progression per year . Over several years, this adds up significantly. Most of the benefit occurs in the first 6–12 months of wear, and the slowed growth effect continues as long as ortho-k is worn nightly. Keep in mind, ortho-k does not reverse existing myopia – it just corrects it temporarily each day and slows further worsening.
Age suitability: Typically ages 8 and up are good candidates (or younger if very responsible with hygiene and lens handling). The child must be mature enough to handle putting lenses in and out and maintaining them. Many 8–12 year-olds do great with ortho-k after a proper training period. Starting around the pre-teen years is common. Ortho-k can be continued into the teens and beyond, or one can switch to daytime contacts later – but if you stop ortho-k entirely, the cornea goes back to its original shape and myopia control benefit stops.
Pros: No glasses or contacts needed in daytime – clear vision all day is a huge plus for active kids or those self-conscious in glasses. It’s effective (~50% progression reduction on average ). It addresses vision and control together. Compliance is easy to monitor – if the child sees well in the morning, you know they wore their lenses. Ortho-k can correct moderate myopia (up to around -6.00 D) and mild astigmatism simultaneously. The treatment is fully reversible – if you stop, eyes return to original shape/prescription.
Cons: Ortho-k requires rigorous lens care. Because lenses are worn overnight, hygiene is paramount to prevent infections (lenses must be cleaned daily, and cases kept sterile). There’s an adaptation period – the first few nights can feel odd, and vision in the first week may fluctuate until the cornea molding stabilizes. Families incur higher upfront costs: the fitting fee and first pair of lenses can be several hundred to over a thousand dollars. However, that often includes follow-ups and replacement lenses for a year. Each year, lenses may need to be refit or replaced, so ongoing costs might be on the order of $500–$1000/year (varies globally). Losing or damaging a lens means an unexpected cost. Also, ortho-k mainly works for mild to moderate myopia; very high prescriptions might not fully correct to 20/20 (though they could still get partial correction and possibly pair with glasses).
Side effects: The main concern is the risk of corneal infection (microbial keratitis), since any overnight contact lens wear slightly increases this risk. However, ortho-k’s safety record in kids is generally good with responsible care. Studies estimate infection rates around 7 per 10,000 patient-years, similar to other overnight lens use . In other words, roughly a 0.1% chance per year. While rare, infections can be serious, so proper lens hygiene and immediate care for any red, painful eye are critical. Some children experience mild lens discomfort or glare/halos (especially if there is residual correction or decentered lens fit). Most adapt quickly and report good comfort during sleep. Regular check-ups ensure lenses fit well to minimize risks. Overall, with modern high-oxygen materials and protocols, ortho-k is considered a safe option for children – no serious adverse events were reported in several multi-year pediatric studies .
Follow-up: Fitting ortho-k involves a few extra visits at the start: after the first night, first week, first month, etc., to check the cornea and vision. Once settled, typically every 6 months the child should have an exam (more frequently if any issues). The optometrist will monitor corneal health, ensure the lenses are still centering and providing the intended effect, and measure any prescription changes. Often they’ll do annual topography maps of the cornea to visualize the lens effect. Parents should also communicate any changes (e.g. if morning vision is not as clear, which could mean lenses need replacement or refitting sooner). As the child grows, new lenses are periodically made to match any eye parameter changes.
Soft Multifocal Contact Lenses for Myopia Control
What it is: These are special soft contact lenses worn during the day (like regular contacts) but designed with optics that slow myopia progression. They typically have a dual-focus or multifocal design: part of the lens corrects the child’s distance vision, while other parts of the lens focus light slightly in front of the retina (creating “myopic defocus”). This simultaneous defocus signal across the retina is believed to inhibit the stimulus for eye elongation, similar to ortho-k’s effect but achieved optically in a soft lens . The most famous example is the CooperVision MiSight one-day lens, which has FDA approval for myopia control in 8–12-year-olds. Other companies have their own versions (some practitioners also use off-label “multifocal” contacts with a +2.00 to +2.50 add power center-distance design, which research has shown can be effective).
Effectiveness: High-quality evidence supports these lenses. In a 3-year randomized trial, children wearing MiSight daily disposables had 59% less refractive myopia progression and 52% less axial elongation than children wearing regular single-vision contacts . Specifically, the MiSight group progressed only -0.51 D over 3 years versus -1.24 D in controls . Axial length growth was 0.30 mm vs 0.62 mm. These are impressive results, essentially cutting progression in half. Follow-up studies up to 6 years suggest the effect persists (and even older kids who started later still benefited). Similarly, the NIH-funded BLINK study found that using a high-add (+2.50) multifocal soft lens slowed 3-year myopia progression by ~43% compared to a single-vision lens . Real-world: if normally a child’s Rx would worsen by -1.00 D per year, these lenses might slow that to ~-0.4 to -0.5 D per year on average. They don’t usually stop progression entirely, but markedly reduce it. For many kids, that can mean ending up several diopters less myopic by their late teens.
Age suitability: Usually around 8–12 years is the prime age to start, as kids in this range can learn to handle daily contact lens wear with supervision. In fact, studies found children as young as 8 adapted well to daily disposable contacts (with proper training, they can insert/remove lenses safely). Starting at or just before the onset of myopia is ideal. Teenagers can also use these lenses; however, myopia tends to slow naturally in later teens, so the biggest benefit is when begun earlier in the rapid phase. If a child isn’t ready for contacts, you might use atropine or glasses first and then switch to MF contacts a couple of years later when they’re more mature.
Pros: Children get excellent vision correction and are often thrilled to be glasses-free during the day. Daily disposable versions (like MiSight) are very convenient and hygienic – no lens cleaning, just use a fresh pair each day. Soft lenses are comfortable once kids adjust – after a week they usually forget they’re in. The myopia control benefit (~30–60% slowing) is significant. There are no pharmaceutical side effects and no overnight wear, so the risk profile is simply that of normal daytime contact lens use (which is low, especially with dailies). Many parents also like that this is a “removable” option – if the child has trouble, you can always stop or take breaks (unlike a surgical approach).
Cons: The child must be responsible enough for contact lens wear – inserting every morning, removing every evening, and not overwearing them. Some younger kids may need help from parents at first. Using contacts is a daily routine that some find too cumbersome or intimidating (though lots of kids do great and feel proud taking care of their lenses). Cost can be higher than standard contacts: MiSight, for example, might run around $750–$1000 per year (since it’s a proprietary lens). However, some practitioners bundle it with check-ups. Off-label multifocal lenses can be cheaper (e.g. monthly lenses replaced quarterly), but then you need a very expert fitting. Another consideration: lenses must be worn consistently (at least 6 days a week, ideally all waking hours) to get full myopia control effect. If a child only wears them occasionally and goes without correction other days, the benefit likely drops. Lastly, while uncommon, some kids may have initial adaptation issues like slight ghosting or reduced contrast due to the multifocal optics. Usually, visual quality in good lighting remains high (20/20 achievable), but low-contrast situations can feel a tad different than single-vision lenses. Proper fitting and lens design choice mitigate this.
Side effects: Largely the same as any soft contact lens wear. With daily disposables, the infection risk is very low (estimated 1 in 5,000 users per year for microbial keratitis in daily lens wear, and milder complications like conjunctivitis or corneal abrasions are infrequent). Parents should supervise younger kids’ lens hygiene. Some children’s eyes may get a bit dry or irritated, but using high-quality lenses and perhaps occasional rewetting drops usually addresses that. There are no systemic effects – the amount of add power in the lens doesn’t affect the body, just the focusing of light. Overall, soft myopia control contacts are considered safe and effective for children when proper guidelines are followed . Many eye doctors report that children are often even more careful than teens or adults with their contacts!
Follow-up: Typically a 1-month follow-up after starting to ensure the lenses fit well, vision is good, and the child is comfortable with handling. Then exams at least every 6 months to track prescription and axial length. If progression is well controlled, no changes needed. If myopia is still creeping up faster than expected, the practitioner might verify lens centration and wear time (or consider combining with atropine in certain cases). Contact lens prescription will be updated as the eye grows (usually each year a slightly stronger power might be dispensed if needed). Because these kids are wearing contacts full-time, regular check-ups are also important to monitor corneal health. If any redness or eye irritation occurs, parents are advised to have the child stop lens wear and see the clinic promptly to rule out any problem. In practice, families on these programs often build a good rapport with their optometrist through regular visits.
Defocus Spectacle Lenses (e.g. HOYA MiYOSMART, Essilor Stellest)
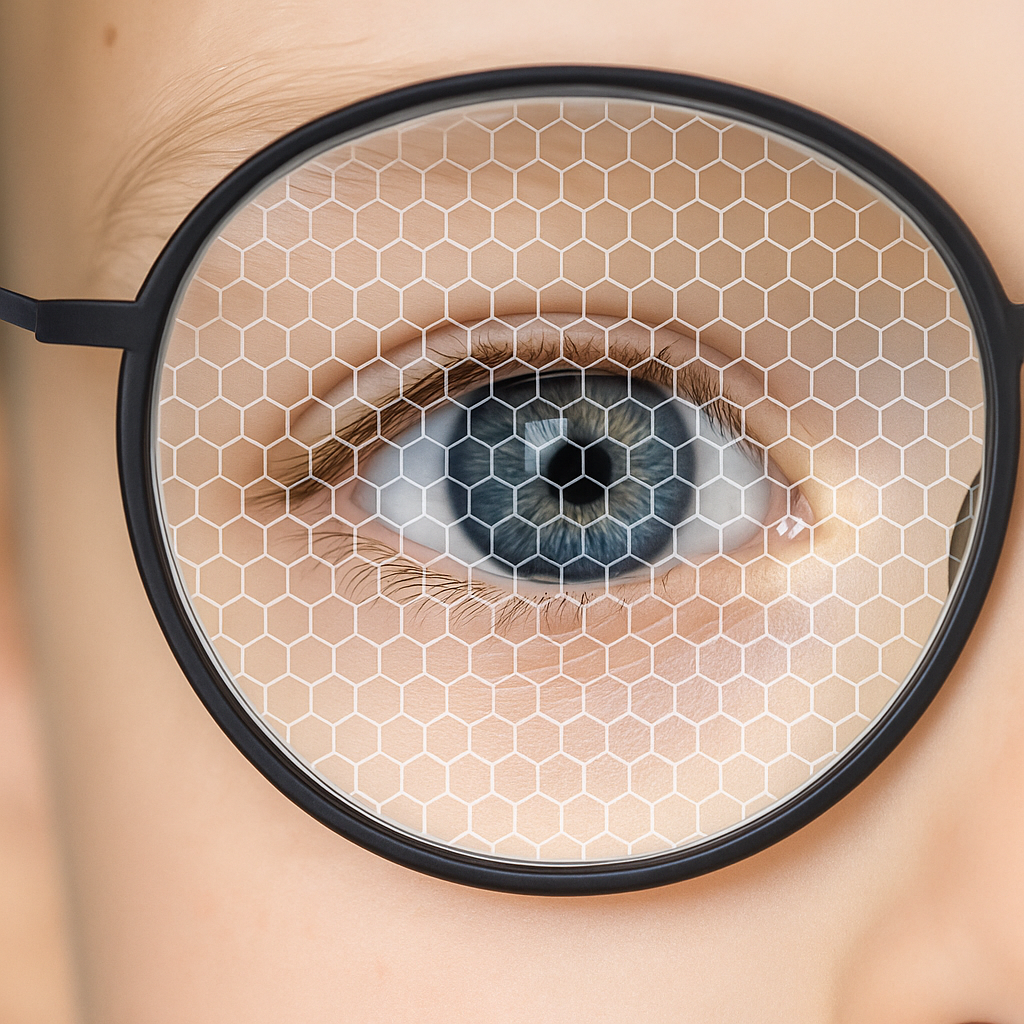
What it is: These are eyeglasses designed specifically to slow myopia progression. They look like normal thin kids’ glasses, but the lens has a special optical layout. For example, the HOYA MiYOSMART lens uses “D.I.M.S.” technology – a honeycomb pattern of tiny lenslets in the periphery that focus light in front of the retina (myopic defocus) while the central zone corrects distance vision. Essilor’s Stellest lens uses “H.A.L.T.” technology – multiple rings of aspherical lenslets to create a volume of defocused light in front of the retina . The central 9mm of the lens is clear for normal vision. Essentially, these lenses provide clear vision and constantly project a defocus signal to the peripheral retina as the child wears them. They are a next-generation update on older ideas like bifocal or progressive glasses (which had limited effects ~10–15%). These new designs show much stronger efficacy.
Effectiveness: Clinical trials are very promising. A 2-year randomized study of the MiYOSMART DIMS lenses showed about 60% less myopia progression on average compared to regular single-vision glasses . Children wearing DIMS lenses progressed roughly -0.3 D in 2 years versus -0.8 D in the control group . Axial growth was similarly slower (around 0.2 mm vs 0.4 mm). Follow-up studies out to 6 years indicate the effect sustains and there’s no rebound if children switch back to normal lenses later . The Essilor Stellest lens trial found that after 2 years, children who wore the lens 12+ hours per day had 67% less refractive progression (0.99 D less) and 60% less axial elongation than controls . Even on average (including those with lower compliance), Stellest still cut progression by ~50% . These numbers rival low-dose atropine and ortho-k outcomes. In practice, it means a child’s prescription might change very little over a year with these glasses, whereas it might have jumped significantly with normal lenses. It’s important to note the wearing time – to get full effect, the child should wear these glasses as much as possible when awake (at school, home, etc.). If they only put them on for part of the day, the benefit may reduce.
Age suitability: Any child who wears glasses can use these specialized lenses. They’re great for young kids (5–7 years) who are myopic but not ready for contacts or other interventions. They’re also ideal if parents prefer a non-invasive, no-maintenance option – it’s just like wearing normal glasses. Because they look and feel normal, there’s no adaptation needed by the child (aside from possibly a brief period to get used to any slight difference in peripheral vision). These lenses can be prescribed as soon as myopia is detected and recommended through the early teens. Even older teens with continued progression could benefit. Essentially, if the child needs vision correction and compliance with glasses is good, this is a very accessible method.
Pros: Very easy to use – just wear glasses as usual. There are no eye drops, no contact lens routines. It’s a non-contact, non-pharmaceutical approach, which appeals to many families. The appearance is indistinguishable from regular lenses; the child won’t have weird-looking glasses (the defocus elements are microscopic). Safety is excellent – it’s just a lens, so no medical side effects. The effectiveness (50–60% slowing) is on par with the best other methods . If a child already likes wearing glasses, this is a seamless upgrade. Also, if for some reason the child isn’t wearing them (say they play sports without glasses), there’s no risk like with forgetting a medication – they just don’t get the benefit during that time.
Cons: The main downside is cost – these lenses are more expensive than standard single-vision lenses. Globally, they might cost a few hundred USD per pair (perhaps 2–3× the cost of regular kids’ lenses). Since children’s prescriptions change, new lenses may be needed yearly or sooner, adding ongoing expense. That said, it’s still generally cheaper than many years of specialty contacts. Another consideration: while these lenses provide good vision, some children might notice slightly reduced clarity in the far periphery or mild ghosting in certain lighting, due to the lenslet structure. Most adapt and don’t have complaints, as the central vision is fully clear . However, if a child is extremely sensitive, it could bother them (this is uncommon). Finally, compliance is key – if a child frequently takes off their glasses (some kids dislike wearing glasses full-time), the myopia control benefit decreases. You need buy-in that the child will actually wear the glasses when needed. For very active kids who keep removing their specs, contacts or atropine might yield better consistent dosing.
Side effects: Virtually none medically. These lenses won’t harm the eyes – they simply change light focus. Eye strain or headaches are not reported beyond what any glasses wearer might experience adjusting to a new prescription. One could argue a “side effect” is that kids must experience some blur in peripheral vision by design; but since the brain mostly pays attention to the central field, children generally tune this out. There’s no restriction like with bifocals (where you had to point your nose to see clearly at certain distances) – these work simultaneously at all gaze angles. Importantly, wearing defocus lenses will not weaken the eyes or make the myopia “worse” – some parents worry that not giving full vision to the periphery could be bad, but studies show the opposite: it’s beneficial for controlling growth .
Follow-up: Standard eye exam cadence, usually every 6 months for myopic kids. The optometrist will check if the prescription changed and can quickly assess axial length changes. Typically, they’d replace the lenses if the child’s Rx increased by ~0.50 D or more, or at least once a year as the child grows (to keep vision sharp). If the child’s myopia is not progressing at all or very slowly, it’s a win – they stay the course. If progression is still faster than desired, ensure the glasses are worn consistently and consider combining with another method (in some cases, doctors do both atropine drops and defocus glasses for an added effect). Thus far, no adverse effects from long-term wear have emerged; children in Hong Kong and elsewhere have worn them 5+ years with continued slowed progression and normal visual function . Families should be reminded to get lenses updated when needed – wearing an outdated prescription won’t hurt the myopia control, but the child won’t see as clearly and might be less inclined to keep them on.
Lifestyle & Outdoor Time for Myopia Control in Children
What it is: Environmental adjustments to help protect against myopia. The two big ones are increasing time spent outdoors (in daylight) and balancing near work (encouraging breaks during long reading or screen use). These are not stand-alone cures for a child who is already myopic, but they can support overall eye health and possibly reduce the rate of progression a little. Notably, plenty of outdoor time (2+ hours a day) has been proven to significantly delay the onset of myopia in children who are not yet myopic . Once a child is nearsighted, outdoor time alone has less dramatic effect on slowing progression , but it’s still recommended as part of a healthy vision lifestyle.
Effectiveness: Prevention: Studies show that kids who spend more time outside have lower chances of becoming myopic in the first place. One long-term study found that an extra 76 minutes of outdoor time per day corresponded to a ~50% reduction in risk of developing myopia . For myopic children, the evidence for slowing progression is mixed – a recent meta-analysis concluded that while outdoor time clearly prevents onset, it “does not seem to slow progression” much in children who already have myopia . Some studies in school programs saw slight benefits, but generally, if a child is growing fast, they likely need one of the optical/pharma interventions to notably alter the course. That said, spending an hour or two outdoors each day certainly won’t hurt and brings other health benefits (exercise, far-distance focus, UV for vitamin D, etc.). It may also somewhat reduce eye strain from constant near activities.
Similarly, reducing excessive near work (especially very close reading distances and marathon sessions of reading/gaming without breaks) is advised. The current thinking: encourage the “20-20-20” rule for screen use – every 20 minutes, look at something 20 feet away for at least 20 seconds – to relax focusing muscles. Ensure good lighting for reading. While these habits alone likely won’t stop myopia progression, they create a more eye-friendly daily routine which, over years, could help at the margins.
Pros: It’s essentially free and healthy. Getting kids outside to play has myriad benefits beyond the eyes (fitness, mood, attention). For eyes specifically, daylight is about 100× brighter than indoor light; this stimulates retinal dopamine release which is thought to slow eye growth . There’s no risk or side effect to outdoor activity (aside from sunburns if not protected!). All myopia experts agree that more outdoor time is recommended for all children, myopic or not. It’s an easy message for opticians to champion to families: “Spend time outdoors each day – it’s one of the best things for growing eyes.” As a complement to other treatments, lifestyle changes can only help. Also, these habits instill long-term visual hygiene that could benefit the child even in adulthood (for example, less digital eye strain, etc.).
Cons: Alone, lifestyle changes usually aren’t enough to control moderate or fast myopia progression. Parents should not feel guilty if their child still needs medical interventions despite more outdoor play – think of outdoors as helpful but not a cure-all. Additionally, increasing outdoor time can be challenging due to weather, safety, or academic schedules (not every family can do 2 hours outside daily, especially in winter or urban settings). It requires conscious effort to change routines. Some children may resist (preferring indoor games or reading). So, while beneficial, it’s not always simple to implement consistently. But even aiming for an extra 30 minutes to an hour outside than before is a good start.
Side effects: Essentially none, aside from maybe scraped knees from playing! Just remember sun protection as needed (hat, UV-blocking eyewear) – ironically, high myopes are at risk of retinal damage from too much sun later in life (due to more light entering a stretched eye), but as kids the focus is on moderate sun for eye growth benefits. There’s also interesting research on using brighter indoor lighting and higher contrast print for near work to mimic some outdoor advantages, but that’s still emerging. The take-home is: let kids be kids and play outside frequently. It’s a natural protective factor for their vision.
Follow-up: Lifestyle advice doesn’t need follow-up in itself, but at each visit, you can gently ask how the child’s daily routine is – “Are you getting outside to play soccer or ride your bike? How many hours of screen time for fun or homework?” Encouraging and tracking improvements can be part of the overall myopia management plan. Some practitioners even have kids keep a log or use a light sensor device in studies, but practically, just keep reinforcing the message each visit. If the child’s progression has slowed, you can praise the role of their healthy habits (along with treatments). If not, it underscores why the other interventions are needed.
Traditional Single-Vision Glasses/Contacts (Monitor Only)
What it is: This is essentially doing nothing special for myopia control, beyond correcting vision. The child wears regular single-vision glasses or contacts to see clearly, and the optometrist monitors their prescription over time. If the myopia worsens, the lenses are updated. This was the standard approach for decades. While it doesn’t actively slow myopia, it’s still the approach for some families who may not opt for specific interventions right away (due to cost, readiness, or uncertainty). It’s important for opticians to understand this baseline, because any myopia control strategy will be judged against the “normal” progression seen with single-vision correction.
Effectiveness: By definition, standard correction has no efficacy in slowing eye growth. In fact, some evidence suggests peripheral hyperopic blur from traditional lenses could slightly hasten progression (one basis for the newer lens designs) . If a child is in single-vision specs, you can expect their myopia to follow its genetic/environmental course – often -0.50 to -1.00 D increase per year in early years (varies widely per child). Some kids progress slower, some faster (e.g., onset at age 6 and -1.00 per year could reach -8 by late teens; onset at 10 and -0.50/yr might end -3.00). There is no intervention to evaluate here, just natural history. It’s worth noting that bifocal or progressive glasses (sometimes tried historically) offer only a small ~10% slowdown – not clinically significant for most, so they aren’t first-line anymore . Thus, plain single-vision or those minor tweaks can be considered essentially the same baseline.
Pros: Simplicity and low cost. Regular glasses are cheapest and easiest to obtain. No extra routines or medications – just come for yearly check-ups. For some families, especially if myopia is mild or just starting, they might choose to “wait and see” before pursuing a treatment. Single-vision correction does provide clear vision, which is of course critical for learning and safety. Some kids prefer glasses or find them fashionable, so they’re happy. If a child’s myopia progression is naturally slow, standard correction with monitoring might suffice (though one can’t predict which child will stay mild vs go high).
Cons: Myopia will likely progress unchecked, potentially leading to a much higher prescription than if a control method was used. There is essentially a lost opportunity to reduce that progression. By the time the child is, say, -5.00, parents might wish they had tried to slow it when it was -2.00. Also, no reduction in future risk – the child is on track for whatever high-myopia risks their genes/environment dictate. From a practice standpoint, doing nothing different means the child will need frequent lens upgrades (cost and inconvenience of new glasses every 8-12 months). Some children get frustrated or anxious as their vision worsens each year (“Mom, my glasses are fuzzy again already”). So while standard care avoids any new hassle, it essentially guarantees the known downsides of progressing myopia.
Side effects: None from the glasses themselves (aside from maybe thicker lenses and the visual distortions those cause at high powers). The “side effect” here is the higher degree of myopia the child will end up with, along with all associated risks of high myopia. That’s not an immediate side effect but a long-term consequence. It’s important to communicate this gently to parents: doing nothing is not neutral – it carries the likelihood of a stronger prescription and higher chance of eye problems later. Sometimes framing it as “active treatment vs. no treatment” helps clarify that standard glasses are not a treatment, just a temporary fix for vision.
Follow-up: Children in single-vision lenses should be seen at least annually, if not every 6 months when in a fast growth phase, to update prescriptions. Frequent exams are the only way to catch big changes and ensure the child isn’t under-corrected (which can affect school performance). Monitoring axial length is less common in routine practice without a myopia program, but some clinics do track it for all myopes now. If progression is faster than expected or the child approaches high myopia, the optometrist might (and frankly should) revisit the idea of starting a myopia control intervention. There’s really no threshold at which it’s “too late” – even starting at -4.00 could slow them from getting to -8.00. So, follow-up is about staying on top of Rx changes and keeping the conversation open about options.
Now that we’ve covered each option, the table below summarizes them for quick comparison, including typical effectiveness, pros/cons, follow-up needs, and cost:
Comparison of Myopia Management Options
To help you counsel parents, here’s a side-by-side look at the key factors:
| Method | How It Works (Mechanism) | Age Fit (Typical Start) |
|---|---|---|
| Atropine Eye Drops (Low-Dose 0.01–0.05%) | Nightly drop slows eye elongation via biochemical signaling in retina/sclera. | ~Age 5–6 and up (early myopes) |
| Orthokeratology (“Ortho-k”) (Overnight Rigid Lenses) | Special RGP lenses worn during sleep reshape cornea temporarily (flatten center) to correct vision & induce peripheral myopic defocus. | ~Age 8–10 and up (responsible with lenses) |
| Soft Multifocal Contacts (e.g. MiSight daily, other center-distance MFCL) | Special concentric or aspheric optics give dual focus: correct central vision + peripheral myopic defocus to slow eye growth. Worn in daytime like regular contacts. | ~Age 8–12 (children can learn contacts) |
| Defocus Spectacle Lenses (Hoya MiYOSMART, Essilor Stellest) | Glasses with lenslet technology: central zone corrects vision, surrounding zones focus light in front of retina (myopic defocus) continuously. | ~Age 5–7 and up (any kid needing glasses) |
| Lifestyle: Outdoor Time & Visual Hygiene | Increase daily outdoor exposure (2+ hrs ideally) to utilize bright light’s protective effect. Encourage breaks during near work (20-20-20 rule) to reduce strain. | All ages (as preventative and adjunct measure for myopes) |
| Single-Vision Glasses/Contacts (Conventional Correction) | Standard lenses that correct vision but don’t alter eye growth stimuli. Light focuses only on retina centrally, peripheral light focuses behind retina. | Any age (this is routine care if no myopia control chosen) |
Costs are broad global estimates in USD for comparison. They vary by region, provider, and insurance. The value of slowing myopia (fewer high-index lenses, lower risk later) often outweighs these costs.
Diagram of a myopic eye versus a normal eye. In myopia, the eyeball is slightly elongated, causing light from distant objects to focus in front of the retina instead of on it. This leads to blurry distance vision until corrected with lenses.
Safety Snapshot: Myopia Control Treatments and Side Effects
Low-Dose Atropine: Extremely safe at 0.01% – pupil dilation is minimal (typically no symptoms). At 0.05%, some kids notice brighter lights or slight difficulty focusing up close, but it’s mild . No systemic effects at these doses. Using photochromic lenses or sunglasses outdoors can help if light sensitivity occurs. Importantly, low-dose atropine has far fewer side effects than the old high-dose 1% atropine (which caused noticeable light sensitivity and near blur). Rebound effect after stopping is minimal at low doses . Overall a well-tolerated long-term option.
Orthokeratology: The primary concern is infection from overnight lens wear. With good hygiene (proper lens cleaning, not wearing when ill or eyes are irritated), the risk of serious infection is low – roughly 1 in 1,000 user-years . For context, that’s comparable to or slightly higher than daily soft lens wear in teens. Parents and kids must adhere to cleaning regimens and attend follow-ups. Other side effects like lens binding or eye abrasions are rare with modern high-oxygen lenses and careful fitting, but can happen – that’s why regular check-ups are required. If the child follows the care instructions, ortho-k is considered safe by eye care professionals worldwide for kids. Always have a plan: if the eye gets red or painful, remove lenses immediately and see the doctor to rule out infection.
Soft MF Contacts: Daily disposables minimize risk – each morning a sterile lens, each night it’s discarded. This avoids lens case contamination issues. Infection in compliant daily lens wearers is very uncommon (on the order of 1 in 5,000 per year). We still teach kids never swim or shower in contacts, and to wash hands before handling lenses. Some children might get minor dryness or irritation – usually fixed by trying a different brand or using rewetting drops. Overall, studies (and now an FDA approval) show these lenses are safe for children as young as 8 with proper supervision. No long-term adverse effect on the eye has been seen; eyes of kids in MiSight trials were healthy after 6 years of wear.
Defocus Glasses: No medical risks. The lens material is the same as regular polycarbonate or high-index lenses, with UV protection etc. A few children might report adaptation symptoms like “weird blur at the side” or slight double vision of peripheral objects in the first days – usually this fades as they adapt to the lens. If a child consistently complains, the optometrist can check fit and ensure they’re looking through the optical center correctly. Safety-wise, these lenses are as safe as any pair of glasses (just be careful with sports, as with any eyewear).
Combination Approaches: Sometimes doctors combine treatments (e.g. low-dose atropine + orthokeratology, or atropine + defocus glasses). Research indicates additive effects and no significant additional risks beyond each component on its own . If using atropine with contacts, the main caution is to put drops in after removing lenses (so lenses don’t absorb the drop). Combination therapy is typically reserved for aggressive cases. Always follow the eye doctor’s guidance on this.
In summary, all these myopia management options have strong safety profiles when properly administered. The key is compliance and communication – following instructions, attending follow-ups, and reporting any issues promptly. As an optician, you can reassure parents that millions of children worldwide are now using these methods safely, and avoiding high myopia is worth it. We always weigh risk vs. benefit: here, the benefits (lower chance of high myopia and its complications) far outweigh the minimal risks of the treatments.
Visualization of a defocus spectacle lens design (Essilor Stellest). The lens has a clear central zone for normal vision, surrounded by rings of microscopic aspherical lenslets. These lenslets create a volume of myopic defocus in front of the retina (illustrated by the white shell), signaling the eye to slow its growth . Despite the complex optics, children report similar visual clarity as with regular lenses.
How to Decide on a Myopia Control Plan – Questions to Guide Parents
Every child and family is different. As the trusted optician, you can help them weigh options by discussing a few key questions:
- “How quickly is my child’s myopia getting worse?” – Faster progression or very early onset (before age 8–9) might warrant a more aggressive approach (like atropine or ortho-k, or even combination). Slower progression or later onset might do well with a single method (like just glasses or contacts with defocus design).
- “What is my child’s lifestyle and personality?” – If they are active in sports and hate glasses, ortho-k or soft contacts could be great so they’re glasses-free in daytime. If they are too young or squeamish about contacts, perhaps start atropine drops and glasses. If they already love a certain modality (e.g. they don’t mind glasses at all), then defocus spectacle lenses are an easy upgrade.
- “Can we commit to the follow-up and routine?” – Some families are very diligent and capable of a complex routine (like nightly lens care for ortho-k). Others might prefer something low-maintenance (like daily disposable MiSight or just putting on a pair of special glasses). It’s important to choose a method that the family can confidently stick with. Consistency = success in myopia control.
- “What are the costs and what does insurance cover?” – Myopia control often isn’t fully covered by basic vision plans, but it varies. Outline the estimated costs of each option over a year or two. Help parents see it as an investment in their child’s vision. For example, ortho-k’s upfront cost might be offset by not needing new glasses yearly. Some clinics offer payment plans or packages. Also mention the long-term cost of very high myopia (special thick lenses, potential medical treatments) that could be avoided.
- “What if we do nothing different?” – Sometimes parents lean toward just updating glasses. It’s worth gently explaining the likely outcome: e.g., “If we continue with regular glasses, based on past trends, Johnny might go from -2 to about -5 by high school. With myopia control, we might keep him closer to -3. This can mean thinner glasses and lower risk to his eyes long-term.” It’s ultimately their choice, but framing the decision with knowledge empowers them.
Encourage parents to ask their own questions. Common ones include: “Is it safe?” (covered above), “How long does my child need to do this?” (usually until late teens or until progression clearly stops), “Will they still need glasses later?” (likely yes, but a much weaker prescription), “Could my child do LASIK eventually?” (possibly, and controlling myopia now will make them a better candidate by keeping Rx lower and eyes healthier).
Frequently Asked Questions (FAQ) – Myopia Control for Kids
Q1: Will my child’s myopia stop if we do these treatments?
A: The goal is to slow down the progression, not necessarily halt it completely. Think of it like slowing a moving car rather than slamming the brakes. On average, treatments can slow myopic worsening by about 30–60%. Your child’s prescription might still change each year, but much less than it would have without intervention . Some lucky children have almost no progression while on treatment, but it varies. The key is, any slowing of growth is beneficial. Even ending up with a prescription of -3.00 instead of -6.00 is a big win for long-term eye health.
Q2: Is one method “best,” or should we combine them?
A: No single method is best for everyone – it depends on the child. All the main options (drops, ortho-k, special contacts, special glasses) have similar efficacy ranges in studies . What’s “best” is the one you can use consistently and safely. Some doctors do combine methods for high-risk cases (e.g. combining atropine with ortho-k for an 6-year-old with -5.00). Combination therapy can have an additive effect , but also more cost/complexity. For most kids, one well-chosen intervention plus good lifestyle habits works great. Your eye doctor will tailor a plan based on factors like age, current prescription, and progression rate. Over the years, the plan may adjust – for example, starting with one approach and adding or switching to another as the child gets older.
Q3: How long will my child need myopia control treatment?
A: Usually until the late teen years when myopia naturally stabilizes. Most progression happens between ages 6 and 16 (with peaks around 8–13). So children often use these interventions for several years. For example, atropine drops might be used for 2 years, then a pause to see if progression has slowed – if not, treatment resumes. Ortho-k and special lenses are typically used all the way through the active progression period (which could be age 18 or beyond in some cases). The doctor will monitor each year; if the prescription hasn’t changed for say 2–3 years in a row and the child is older (late teens), they might “graduate” from the myopia control program. It’s not usually lifelong – it’s meant to cover those growing years. Stopping too early can lead to rebound progression (especially with atropine ), so doctors tend to continue until they’re confident the eye’s growth has naturally slowed.
Q4: Are these treatments new? How do we know they work?
A: Myopia control as a field has exploded in the last decade, but it’s built on longer research. Orthokeratology has been around since the 1990s and studied extensively in the 2000s. Atropine eye drops were first studied for myopia in the early 2000s (the big ATOM trial in Singapore) and have over 15 years of follow-up data . Multifocal contacts were tested in trials like BLINK and got FDA approval (MiSight in 2019) after strong results . Defocus glasses like MiYOSMART and Stellest came out in the last 5–6 years, with large clinical trials confirming their efficacy . So while some products are relatively recent, they are supported by high-quality evidence (randomized clinical trials around the world). Eye care organizations (like the International Myopia Institute and major optometry associations) now endorse these as standard of care options. You’re not guinea pigs – millions of kids globally are benefiting from these tools already.
Q5: What if my child is already a teen or has high myopia – is it too late to start?
A: It’s never too late to attempt slowing things down, though earlier is better. Myopia typically slows in the late teens, but if your 15-year-old is still progressing, an intervention could help squeeze out a bit less growth in those last active years. High myopia (-6.00 and above) especially is worth managing even if late – atropine, for instance, might still reduce some further elongation and thus reduce risk of retinal issues. The percentage benefit might be smaller in later teens, but some benefit is better than none. Also, teens can often handle contacts or ortho-k more responsibly than younger kids, which helps. Of course, we set realistic expectations: a 17-year-old who’s -8.00 already won’t go back to -4.00; we’re just trying to maybe keep them from -9.00 by age 19. If someone is in their 20s, their eye growth is likely done, so myopia control isn’t needed (other refractive solutions might be considered). But for any school-aged child or adolescent with worsening myopia, it’s worth discussing options rather than just watching it happen.
Q6: Will my child still need glasses or contacts in the future?
A: Yes, likely they will still be nearsighted (myopia control doesn’t reverse myopia, it slows it). The aim is that they will need weaker glasses than they would have otherwise. For example, instead of ending up needing -8.00 glasses, they might end up in -4.00 glasses. They will still rely on some form of correction to see distance clearly, unless they choose vision correction surgery in adulthood. The good news is that by keeping the prescription lower, their glasses will be thinner, and if they do consider LASIK in their 20s, it’s more likely to be within treatable range. Some parents ask, “Could this make my child not need glasses anymore?” – the answer is no, it’s not a cure to get rid of today’s glasses (except ortho-k does give daytime clear vision, but that’s like a retainer effect). The focus is on the future. Think of it like managing cholesterol – you’re not eliminating it, but controlling it so it doesn’t cause bigger problems later. And remember, lower myopia is easier to handle in daily life and much safer for the eyes long term.
Q7: What about screen time – did phones/tablets cause my child’s myopia?
A: Excessive near work (including screens) is a contributing factor, but usually in combination with genetics and lack of outdoor time. It’s normal nowadays for kids to have more near tasks. We can’t pin it on any one device, but studies do show children who spend more time on close work and less time outdoors are more likely to become myopic . The pandemic period saw a jump in myopia cases, presumably because kids were cooped up indoors on screens. That said, once a child is myopic, reducing screen time alone won’t magically fix it. It’s more about balance: encourage breaks, good posture, and getting outside after school. Using myopia control lenses or drops will directly help slow the eye’s growth even if school and homework still demand screen use. So yes, screen habits likely played a role and we address that with lifestyle advice, but don’t feel guilty – we have tools to deal with the outcome. Think prevention for younger siblings (more outdoor play can delay onset) and management for the child who is already myopic.
Q8: How do I explain this to my child and get them on board?
A: Great question – a treatment plan is only as good as the child’s cooperation. For younger kids, use simple concepts: “These special glasses/contacts/drops will keep your eyes healthier so you won’t need super thick glasses later.” You can frame it like a team effort – the doctor, the parents, and the child are all working together to “keep your eyes strong.” Kids tend to be quite adaptable. If it’s contact lenses, many 8–10 year-olds find it cool once they succeed in putting them on. For ortho-k, the idea of superhero lenses that work while you sleep can be exciting. Atropine drops might be the toughest sell for some kids (nobody likes drops), but you can make it part of bedtime routine (like brushing teeth). Many kids get used to it – perhaps give a small reward or sticker chart for cooperation initially. Involve them in tracking progress: some practices show kids their axial length graphs going up slower, which can motivate science-minded teens. Also emphasize the short-term perks if any (like “no more glasses during soccer” with ortho-k or contacts). Generally, once kids experience the benefits (clear vision, or pride in taking care of their own lenses), they take ownership. But be patient through the learning curve of any new routine. A supportive, positive approach works better than a coercive one. If a child really resists one method, talk to your eye care provider about trying another – there’s usually a workaround that will suit the child better.
Conclusion & Next Steps: Empowering Families and Protecting Young Eyes
Childhood myopia can feel scary for parents – no one likes hearing their child’s vision is deteriorating. But as we’ve detailed, there’s a bright side: we now have an array of proven tools to help slow down myopia progression. Opticians are in a prime position to guide families through these options with clarity and compassion. By translating the science into simple terms and sharing relatable examples, you help parents make informed decisions they feel good about.
Remind families that myopia control is a long-term partnership. Regular check-ins, adherence to the chosen treatment, and honest communication about what’s working or not are key. The reward is likely a much lower prescription than the child would have had – and that means thinner glasses, potentially easier candidacy for contacts or LASIK in adulthood, and most importantly, a reduced risk of serious eye diseases later on. As the saying goes, ounce of prevention is worth a pound of cure.
Finally, don’t forget to introduce how new technologies can support them in this journey. For instance, once a myopia management plan is set by the optometrist, your role might include helping the family with practical aspects like getting the right eyewear. This is where Optigrid can assist: after the exam, if the child needs new myopia control glasses (say MiYOSMART or Stellest), Optigrid’s remote Pupillary Distance (PD) and segment height measurement tool can ensure those specialized glasses are made with precision. Families can conveniently measure their child’s PD at home using our Virtual Pupilometer – no extra office trip, just a quick photo upload with a reference object. The result is accurate centration of lenses, which is crucial for these defocus designs to work effectively. And for children needing progressive or bifocal segments (in other cases), getting segment height right is equally important – Optigrid handles that remotely too.
Call to Action: Empower your practice and your patients – try Optigrid’s Virtual Pupilometer to seamlessly fit myopia control lenses with confidence. It’s an innovative, easy-to-use platform that complements your clinical care (while never replacing the need for a proper eye exam). With Optigrid, you can offer families the convenience of online eyewear ordering without worrying about PD accuracy, freeing them from extra trips and giving you peace of mind that their child’s new glasses will perform their best. Learn more about Optigrid’s remote PD measurement here and consider integrating it into your myopia management services. It’s one more way to modernize your optical practice and provide top-notch care.
Together, through education, the latest myopia control strategies, and smart tools like Optigrid, we can help the next generation see a clearer future – with healthier eyes and happier parents.
Disclaimer: This article is for educational purposes and is not a substitute for professional medical advice. Always consult an eye care professional (optometrist or ophthalmologist) to determine the best course of action for an individual child. Myopia management plans should be personalized by a clinician. Compliance with treatments and regular monitoring are essential for safety and efficacy. The content here aims to support opticians in understanding current options and communicating them effectively, but final treatment recommendations and medical decisions rest with licensed eye doctors in consultation with the family.

I am a seasoned software engineer with over two decades of experience and a deep-rooted background in the optical industry, thanks to a family business. Driven by a passion for developing impactful software solutions, I pride myself on being a dedicated problem solver who strives to transform challenges into opportunities for innovation.